
A DAN Boater Travel Health and Safety Guide
As you travel and enjoy aquatic environments, you may have the opportunity to observe and interact with marine life. While injuries are rare and usually prompted by human action, we nevertheless face the risk of stings, bites or cuts from marine life any time we enter the water or even walk on the beach. In most cases, injuries are mild and require only simple first aid.
The following sections of this guide cover a variety of injuries and illnesses that travelers may encounter both below and above the water along with tips for preventing injuries and providing first aid.
— Contributors —
James M. Chimiak, MD
Matias Nochetto, MD
An envenomation is the process by which a venom or toxin is injected into another being via a bite, puncture or sting. It is always due to direct contact with an animal or its parts, such as drifting jellyfish tentacles. Two mechanisms of injection are possible: active (such as with jellyfish or cone snails) or passive (such as with lionfish or sea urchins).
Injuries typically occur by incidental contact or deliberate attempts to handle a specimen. Envenomations are rare but can be life-threatening and may require a rapid first-aid response. This guide covers some common envenomations as well as some of the more rare, but serious, cases.

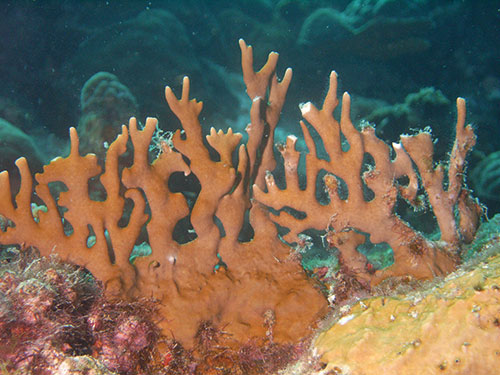
Fire corals, which belong to the genus Millepora, are named for the fiery sensation people have experienced after coming into contact with a member of the genus. They can vary in size from a few inches to more than 2 feet tall.
Fire corals generally have a yellow-green or brownish branchy formation, although their external appearance often varies due to environmental factors. Because fire corals can colonize hard structures, they can adopt a rather stony appearance with rusty coloration.
Despite their calcareous structure, fire corals are not a true coral; they are closely related to Portuguese man-of-war and other hydrozoans.
The mild to moderate burning sensation is the result of cnidocytes (specialized cells) embedded in the corals’ calcareous skeleton. These cnidocytes contain nematocysts, a subcellular structure, which will fire when touched, injecting venom into the victim.
Fire corals are found in tropical and subtropical, often shallow, waters around the world. Individuals who dive or swim in these areas without wearing a wetsuit or dive skin, even when exercising great care around corals, are susceptible to fire coral stings on exposed skin.
The burning sensation may last several hours and is often associated with a skin rash that appears minutes to hours after contact. The acute skin reaction will often subside in a day or two, but it may reappear several days or weeks after the initial rash disappeared.
Lacerations, in which an open wound receives internal envenomation, are the most problematic fire-coral injuries. Venom from Millepora spp. is known to cause tissue necrosis on the edges of a wound. These injuries should be carefully observed, as necrotic tissue provides a perfect environment to culture serious soft-tissue infections.

The blue-ringed octopus (Hapalochlaena maculosa) rarely grows larger than 8 inches (20 centimeters). Their most distinctive feature is the blue iridescent rings that cover their #fcfcd2 body; it is important to emphasize, however, that this feature is displayed only when the animal is disturbed, hunting or mating. When calm or at rest, the animal may display an overall yellowish, gray or beige coloration without any visible blue rings. The blue-ringed octopus is more active at night, spending most of the day hidden in its nest in shallow areas or tide pools.
As with all cephalopods, octopi have a strong beak similar to those of parrots and parakeets. All octopi have venom to paralyze their victims, but the blue-ringed octopus bite contains an extremely powerful neurotoxin called tetrodotoxin (TTX), which can be up to 10,000 times more potent than cyanide and can paralyze a victim in minutes. Theoretically, a little more than 0.5 milligrams of this venom — the amount that can be placed on the head of a pin — is enough to kill an adult human.

Certain bacteria present in the salivary glands of the blue-ringed octopus synthesize the toxin. TTX is not unique to the blue-ringed octopus; certain newts, dart frogs, cone snails, and pufferfish can also be a source of TTX intoxication, although from different mechanisms.
Blue-ringed octopus envenomations are rare. These animals are endemic only to southern Japan, Australia, and the western Indo-Pacific. Cases outside of this region are generally due to the deliberate handling of aquarium specimens. Full recovery is expected with timely professional medical intervention; only a few fatalities have been reported.
A blue-ringed octopus bite is usually painless or no more painful than a bee sting; however, even painless bites should be taken seriously. Neurological symptoms dominate every stage of envenomation, manifesting as paresthesia (tingling and numbness) and progressing to paralysis that could potentially culminate in death.
Signs and symptoms, which usually start within minutes of envenomation, may include paresthesia of the lips and tongue, usually followed by excessive salivation, trouble with pronunciation (dysarthria), difficulty swallowing (dysphagia), sweating, dizziness, and headache. Serious cases may progress to muscular weakness, incoordination, tremors, and paralysis. Paralysis may eventually affect respiratory muscles, which can lead to severe hypoxia with cyanosis (blue or purple tissue discoloration due to insufficient oxygen in the blood).

No antivenom is available, so care is supportive.
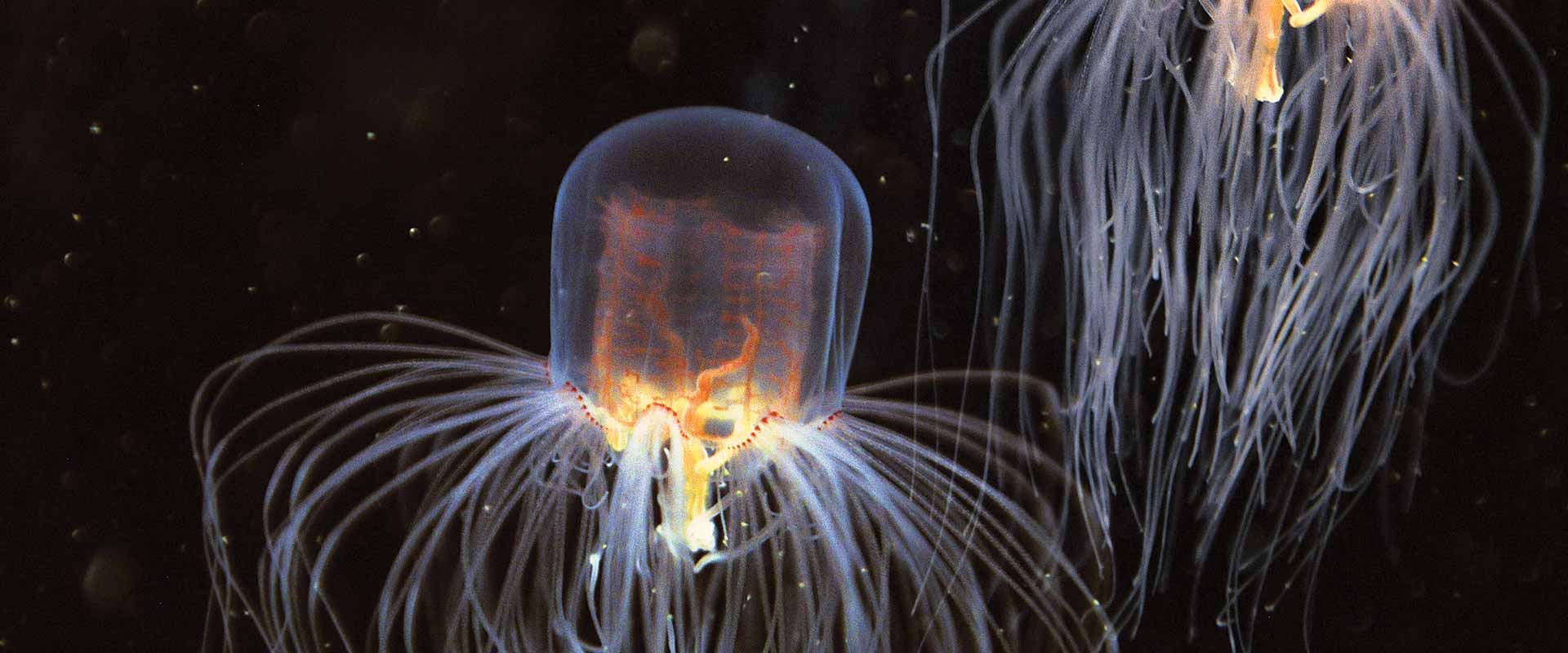
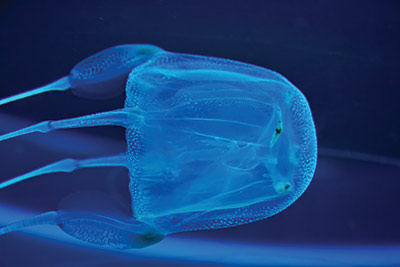
Box jellyfish (class Cubozoa) are cube-shaped medusas — the migrant form of cnidarians — notorious for possessing one of the most potent venoms known to mankind. Certain species can kill an adult human in as little as three minutes, scarcely enough time for any rescue response.
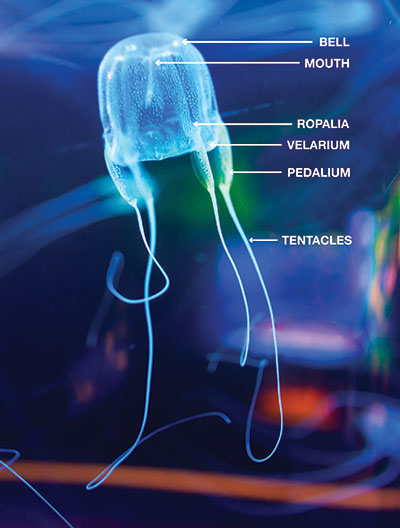
Box jellyfish have a cube-shaped, bell-like body (therefore called cubozoans), with tentacles extending from each corner. They are complex animals with a propulsion mechanism and a relatively sophisticated nervous system for a jellyfish. Some species have up to 24 eyes, some of them with corneas and retinas, enabling them to not only detect light but also see and circumnavigate objects to avoid collision.
While some jellyfish live off of symbiotic algae, box jellyfish prey on small fish, which are immediately paralyzed upon contact with the tentacles. The box jellyfish then retracts the tentacles, carrying the prey into the bell for digestion. Some species hunt daily, and at night one can observe some species resting on the ocean floor.
Contact with box jellyfish triggers the most powerful and lethal envenomation process known to science. As with all cnidarians, the mechanism of injury is the result of myriad microinjections caused by cnidocytes present in their tentacles; these cnidocytes contain nematocysts, a subcellular structure that will fire when touched, injecting its venom.
From 1884 to 1996, there were more than 60 reported fatalities from box-jellyfish stings in Australia. Species of box jellyfish are in almost all tropical and subtropical seas, but life-threatening species seem to be restricted to the Indo-Pacific region.
Sea wasp. Found in the coastal waters of Australia and Southeast Asia, sea wasp is the common name for the most dangerous cnidarian: Chironex fleckeri. The largest cubozoan, sea wasps have a bell approximately 8 inches (20 centimeters) in diameter and tentacles ranging from a few centimeters to up to 10 feet (3 meters). Contact with these animals can result in death. Sea-wasp envenomation causes immediate excruciating pain, which is sometimes followed by acute fatal cardiac failure. Death may occur in as little as three minutes after contact.
Studies have identified a component of the venom that drills a hole in red blood cells, causing a massive release of potassium (hyperkalemia), possibly responsible for the lethal cardiovascular depression. The same study may have also identified a way to inhibit this effect, which in the coming years might prove to be clinically promising.
Four-handed box jellyfish. The four-handed box jellyfish (Chiropsalmus quadrumanus) habitat spans from South Carolina to the Caribbean, the Gulf of Mexico and as far south as Brazil. The four-handed box jellyfish, which can inflict extremely painful stings, is the slightly smaller American cousin to the Australian sea wasp. There is one documented case of a 4-year-old boy who was stung in the Gulf of Mexico and died within 40 minutes.
Bonaire banded box jellyfish. The Bonaire banded box jellyfish (Tamoya ohboya) is a relatively unknown, highly venomous species usually found in the Dutch Caribbean. Since 1989 there have been roughly 50 confirmed sightings primarily in Bonaire, with the remainder on the shores of Mexico, St. Lucia, Honduras, St. Vincent and the Grenadines. Of the three properly reported cases of envenomation, which led to intense pain and skin damage, only one case required hospitalization.

If stung by any jellyfish, follow these procedures in this order:
Tiny box jellyfish found near Australia, Carukia barnesi and Malo kingi, are responsible for the infamous and extremely painful symptomatic complex known as Irukandji syndrome. These small cubozoans’ bells measure only a few millimeters (0.1 inches) with tentacles up 3 feet (1 meter). Fortunately, fatalities from these smaller species are rare, but stings are extremely painful and can cause systemic symptoms, including cardiovascular instability, which should prompt immediate medical attention. Survivors have reported a feeling of impending doom, claiming they were certain that they could not survive such intense, generalized pain; it is important to emphasize, however, that a single sting should not be fatal.
Although probably less dramatic, Irukandji-like syndromes have been reported in other parts of the world, always within marine tropical environments. Species have not been identified, but small species of cubozoans may be the culprit.
Although stings from lesser-known species of cubozoans are not necessarily lethal, they can still be very painful. An immediate medical evaluation is always recommended.


There are about 600 different species of cone snails, all of which are venomous. Cone snails live in shallow reefs, partially buried under sandy sediments, rocks or corals in tropical and subtropical waters. Some species have adapted to colder waters.
Injuries typically occur when the animal is handled. Cone snails administer stings by extending a long flexible tube called a proboscis and then firing a venomous, harpoonlike tooth (radula).
The prevalence and incidence of cone-snail envenomations are unknown, but it is probably a very rare occurrence. Shell collectors (professional or amateur) may be at higher risk.
A cone-snail sting can cause mild to moderate pain, and the area may develop other signs of acute inflammatory reactions such as mild redness and swelling. Conotoxins affect the nervous system and are capable of causing paralysis, which could lead to respiratory failure and death.

There is no specific treatment for cone-snail envenomations. First aid may focus on controlling pain but might not influence outcomes. Envenomation will not necessarily be fatal, but depending on the species, the amount of venom injected and the victim’s body size and susceptibility, complete paralysis may occur, which may lead to death. Conesnail venom is a mixture of many different substances, including tetrodotoxin (TTX).
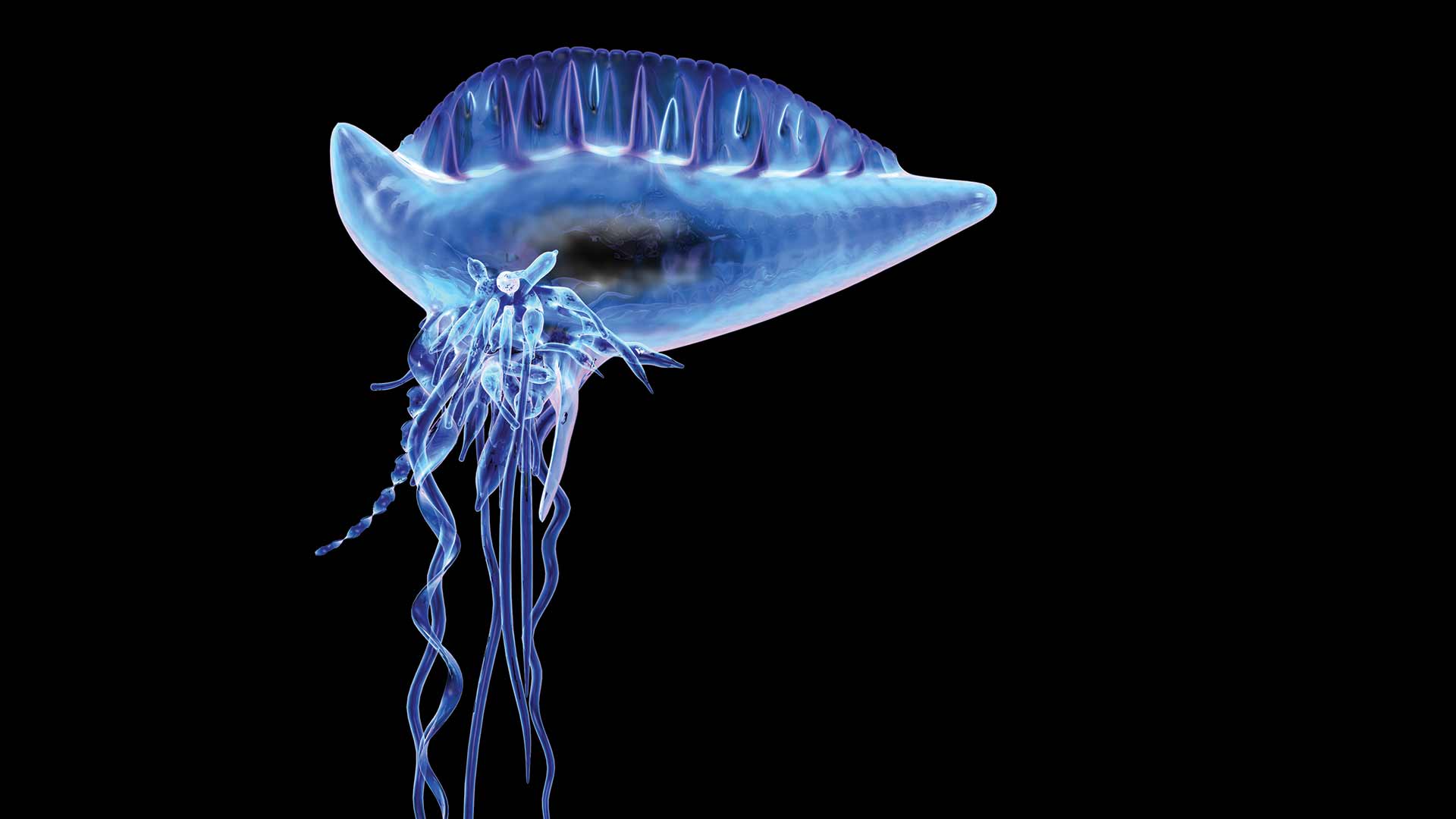
The Portuguese man-of-war is a free-floating cnidarian characterized by blue gas-filled bladders and long tentacles that drift on the surface of the ocean. Contact with a man-of-war’s tentacles can cause intense pain and other systemic symptoms.
This genus has two species: Physalia physalis in the Atlantic and Physalia utriculus (also called bluebottle) in the Indo-Pacific. The Atlantic species may reach slightly larger dimensions, with the gas bladder rarely exceeding 1 foot (30 centimeters) and tentacles averaging 33 feet (10 meters), possibly extending up to 165 feet (50 meters).
Although many people mistake the Portuguese man-of-war for a species of jellyfish, this genus belongs to the order Siphonophorae, a class of hydrozoans. What at first appears to be a single specimen is actually a colony composed of up to four different types of polyps. Despite its resemblance to jellyfish, these animals are more closely related to fire corals.
The Portuguese man-of-war is easily recognizable: If you see blue tentacles, they most likely belong to Physalia.
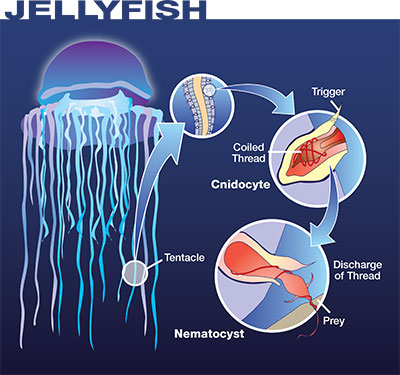
Contact with a Portuguese man-of-war can trigger an extremely painful envenomation process. As with all cnidarians, the mechanism of injury is the result of myriad microinjections caused by cnidocytes present in their tentacles; these cnidocytes contain nematocysts, a subcellular structure that will fire when touched, injecting its venom.
The man-of-war’s polyps contain cnidocytes that deliver a potent proteic neurotoxin capable of paralyzing small fish. For humans, most stings cause red welts accompanied by swelling and moderate to severe pain. These local symptoms last two to three days.
The Portuguese man-of-war causes the most cnidarian envenomations that prompt emergency evaluation globally. Approximately 10,000 cnidaria envenomations occur each summer off the coasts of Australia, the vast majority of which involve Physalia. Most Physalia stings occur on beaches or on the water’s surface rather than while submerged, so the envenomation risk is less for divers. Certain regions are known to have seasonal outbreaks, but incidence is highly variable among regions.
Systemic symptoms are not frequent but can be severe. They may include generalized malaise, vomiting, fever, elevated heart rate at rest (tachycardia), shortness of breath and muscular cramps in the abdomen and back. Severe allergic reactions to the man-of-war’s venom may interfere with cardiac and respiratory function, so anyone envenomated should always seek a timely professional medical evaluation.


Vinegar use is controversial with Physalia spp. Although the use of vinegar has traditionally been recommended, some studies — both in vivo and in vitro — show massive nematocyst discharge upon pouring household vinegar over certain species of cnidarians, including Physalia. The most current American Heart Association guidelines (AHA 2015), however, recommend application of vinegar for all jellyfish stings, including from Physalia spp. DAN Boater will provide updates if the recommendations change.
If you choose to apply vinegar, use spray bottles to optimize application. Generously spray the affected area with vinegar and let it sit for at least 30 seconds to stabilize any remaining cnidocytes. Use tweezers or gloves to pick off any remaining tentacles.

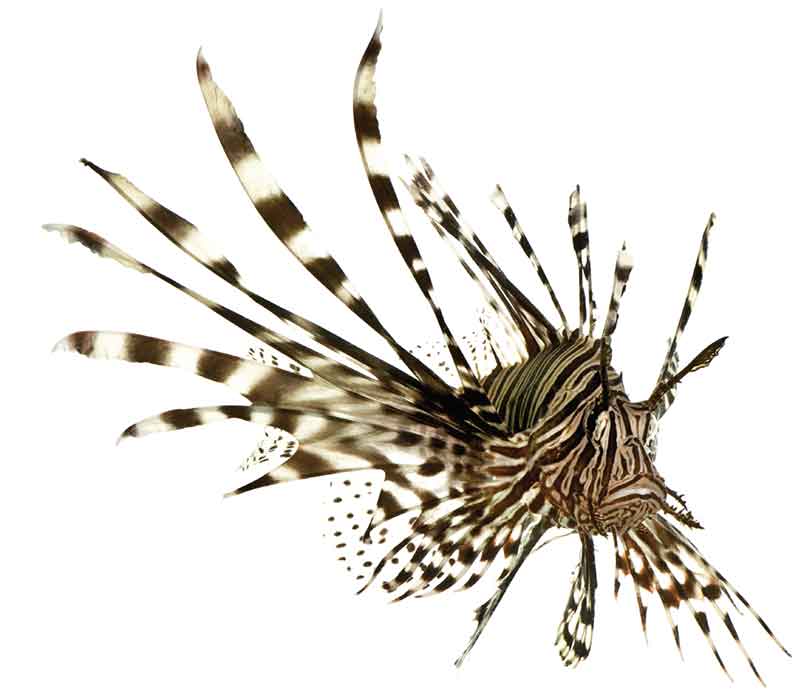
Lionfish, turkeyfish, and zebrafish are common names for fish species of the genus Pterois, a subset of fish of the venomous Scorpaeniformes order. Though lionfish are native to the Indo-Pacific, members of the Scorpaenidae family can be found in oceans all over the globe, even in arctic waters. Lionfish specimens are typically red with white and black stripes and have showy, spiky fins. Species include Pterois volitans, Pterois miles, Pterois radiata and Pterois antennata, among others.
Since the early 1990s, invasive lionfish have wreaked havoc on local juvenile reef fish populations in the western Atlantic. Out of the 11 species of Pterois, only Pterois volitans and Pterois miles are found in western Atlantic waters, but they range from as far north as Rhode Island to the Caribbean basin and down to Brazil.
Knowing no predators, lionfish are generally docile, allowing humans to approach closely enough to make them easy targets for spearfishing. Unfortunately, the desperate attempts to eradicate these fish from the Americas have caused a significant rise in the incidence of lionfish puncture wounds.
Most lionfish-related incidents occur as a result of careless handling, usually during spearfishing or while preparing them for consumption. Lionfish have needlelike spines located along the dorsal and anal fins.
The prevalence and incidence of lionfish envenomations are unknown. Treating physicians may choose to not consult a poison control center, and in the United States they are under no obligation to report these injuries to state or federal agencies. Scientific literature accounts for 108 cases of lionfish envenomations reported between 1976 and 2001, and most of these reports are from marine aquarists. It is impossible to know how often victims go untreated and how often treatment goes unreported, but the frequency of case reports seems to indicate that lionfish envenomations are not uncommon.
Lionfish culling tournaments are becoming popular all over the Caribbean. Recent studies conducted by DAN staff from Cozumel, Mexico, accounted for 26 cases of lionfish envenomation over the first four years of tournaments. Incidence of injury during these events was between 7 and 10 percent of participants.
Lionfish punctures can be extremely painful and lead to the rapid development of localized edema and subcutaneous bleeding. Pain can last for several hours, edema typically resolves in two to three days, and tissue discoloration can last up to four or five days. Due to edema and the venom’s inherent toxicity, puncture wounds on fingers can lead to ischemia (restriction of blood supply to the tissues) and necrosis.

Bites account for the majority of trauma associated with marine life. Fortunately, serious encounters are extremely rare. Traumatic injuries are usually the result of an animal’s defensive reaction to a perceived threat or misidentification of a person’s body part as a food source. Most puncture wounds do not contain venom and therefore are a traumatic injury. Bleeding is the most common acute complication to trauma, and infections are the most common secondary complication. This section covers the more common traumatic injuries, how to prevent them and how to properly manage them.

Skin abrasions, minor skin cuts and scrapes are very common. Accidental contact with rocks, corals, debris and other hard surfaces in or around water can cause injury. Although not common, some superficial wounds that occur in watery environments could become infected with Mycobacterium marinum — which may cause the disease known as aquarium granuloma — especially when the scratch does not properly heal after weeks of what seemed to be proper wound care.
Spending time in or near the water exposes you to the possibility of abrasions because of low visibility within the water and wet and slippery environments. Be aware of your surroundings, and move with caution.
In case of minor skin abrasions, follow these basic first-aid guidelines:
If bleeding has been controlled, do the following:
If bleeding persists, do the following:
For abrasions or amputations with significant bleeding, immediately contact local emergency medical services, apply bleeding-control techniques, and monitor the victim’s vital signs. Be prepared to manage shock.
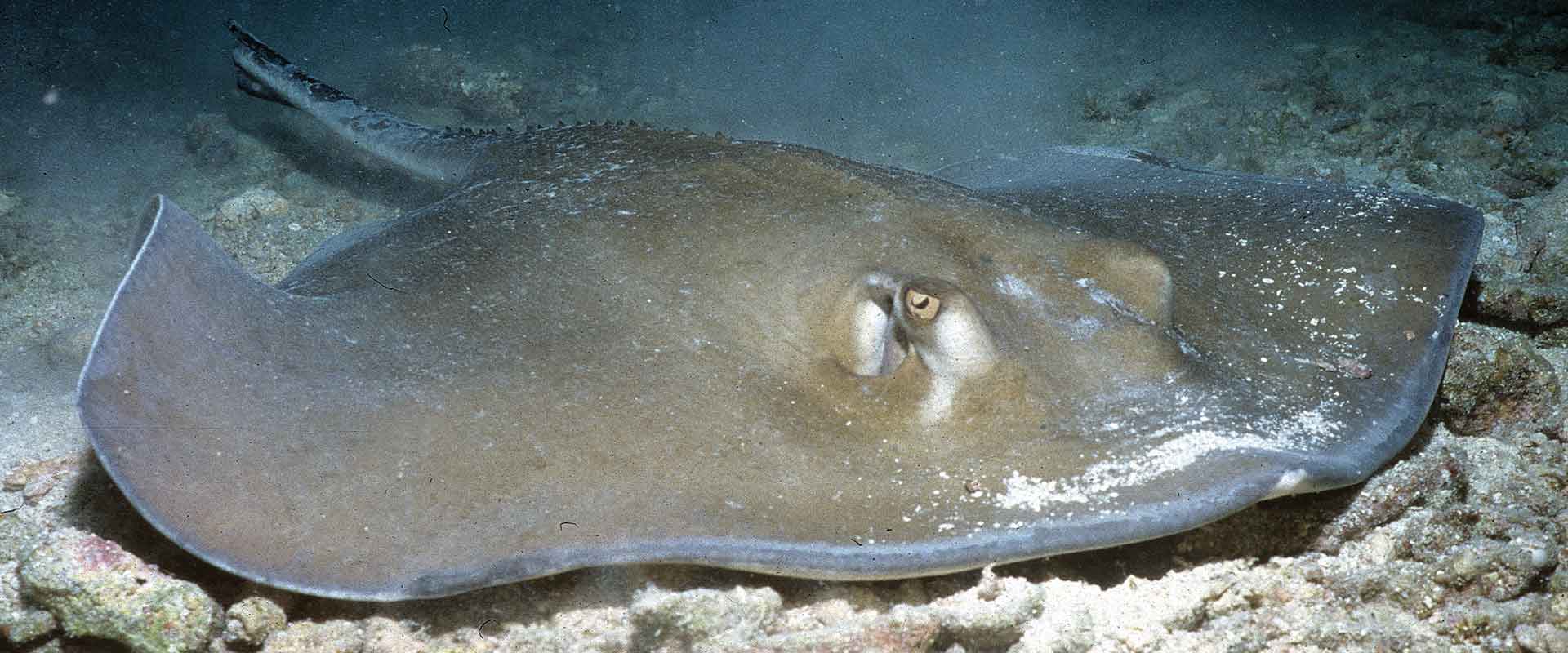
Rays are closely related to sharks: Both are in the class Chondrichthyes (chondr- meaning cartilaginous and -ichthyes meaning fish). Not all rays have stingers. Stingrays are a specific group of rays classified in the suborder Myliobatoidei, which consists of eight families: deepwater stingrays, river (freshwater) stingrays, sixgill stingrays, whiptail stingrays, butterfly rays, eagle rays, round rays and stingarees.
The approximate stingray wingspan varies across species from 1 foot (0.3 meters) to more than 6 feet (1.8 meters). Some freshwater species can weigh up to 1,300 pounds (600 kilograms).
Species of stingrays are in nearly all oceans. Some families consist of only freshwater species, which are typically found in tropical, subtropical and temperate river environments.
Stingrays are not aggressive, and injuries are rarely fatal. The stingray’s defense mechanism consists of a serrated barb at the end of its tail, with venom glands located at the base of the barb. The venom is a variable mixture of substances, none of which are specific to the animal; therefore, the creation of antivenom is not possible. Stingrays will strike when threatened or stepped on. The barb can easily tear wetsuits and penetrate skin and may cause deep, painful lacerations.
Stingrays are responsible for an estimated 1,500 accidents each year in the United States. Prevalence in other countries might be higher, particularly injuries associated with freshwater species, but epidemiological data is either elusive or nonexistent.

Stingrays can inflict mild to severe puncture wounds or lacerations. The initial symptom is pain, which can be significant and intensify over several hours. Both puncture wounds and lacerations can damage major blood vessels, causing severe, potentially life-threatening bleeding. The barb usually breaks off, and removal may require professional surgical care.
It is common for stingray wounds to become infected despite proper care. Possible infections include cellulitis, myositis, fasciitis and tetanus.

Sea urchins are echinoderms, from Echinodermata — a phylum of marine animals shared with starfish, sand dollars and sea cucumbers. Echinoderms are recognizable because of their pentaradial (five rays) symmetry, which is easily observed on starfish. This symmetry corresponds with a water-vascular system used for locomotion, respiration and transportation of nutrients and waste.
Sea urchins have flexible tubular feet that enable movement. Some sea urchins have toxic claws called pedicellariae, which can inflict a relatively painful envenomation, although usually no worse than a bee sting or ordinary jellyfish sting.
Sea urchins feed on organic matter in the seabed. Their mouth is located on the base of their shell, and their anus is on the top. The color of sea urchins varies depending on the species — shades of black, red, brown, green, yellow and pink are common.
Species of sea urchins are in all oceans, from tropical to arctic waters. Most incidents between humans and sea urchins occur in tropical and subtropical waters.
Sea urchins are covered in spines, which can easily puncture the skin and break off. These spines are made of calcium carbonate, the same substance contained in eggshells. Sea-urchin spines are usually hollow and can be fragile, particularly when extracting broken spines from the skin.
Injuries usually happen when people step on sea urchins on while walking across shallow rocky bottoms or tide pools. People are often injured while swimming on the surface in shallow waters as well as when entering or exiting the water.

Although little epidemiological data are available, sea-urchin puncture wounds are relatively common, particularly for people in shallow waters, near rocky shores or in close proximity to wrecks and other hard surfaces. DAN medical information specialists receive at least one call a week regarding sea-urchin injuries, typically from people swimming in very shallow waters near rocky shores.
Injuries are typically in the form of puncture wounds, often multiple and localized. Skin scrapes and lacerations are also possible. Puncture wounds are generally painful, with redness and swelling. Pain ranges from mild to severe depending on several factors, including the species of sea urchin; the body area of the wound, joint or muscular layers compromised; number of punctures; depth of punctures and the individual’s pain threshold. Multiple puncture wounds may cause limb weakness or paralysis, particularly with the long-spined species of the genus Diadema. On very rare occasions, life-threatening complications may develop.
There is no universally accepted treatment for sea-urchin puncture wounds. Both first aid and definitive care are symptomatic.
Contrary to popular belief, very few species of sea urchins are toxic. Pain and swelling are often the result of the body’s reaction to myriad antigens present on the surface of the spines.
Spines are usually covered with strong pigments, so individual puncture wounds are often clearly visible and may cause suspicion that each puncture contains a fragment of a spine. Though this is possible, it may not necessarily be the case. It is easier to assess each individual puncture once the acute inflammatory process has started to recess.
The decision of whether surgical removal of retained spines is necessary is usually based on joint or muscular layer involvement and whether there is pain with movement or signs of infection. Spines will usually encapsulate in a short time, but they may not always dissolve. A reactive granuloma is a common reaction to remaining small foreign bodies. Radiological localization, fluoroscopy or an ultrasound might be useful to avoid a blind surgical extraction that may cause further spine fracture.
Anti-inflammatories and physical therapy are often keys for managing these injuries, particularly when they involve small joints, because a prolonged inflammatory process may result in fibrosis, which may limit range of motion.
If signs of infection are present, the doctor may prescribe antibiotics and a tetanus booster.
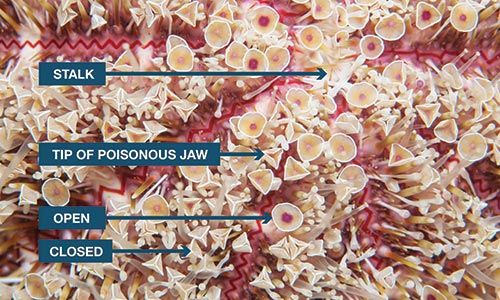
The flower sea urchin (Toxopneustes spp.) is the most toxic of all sea urchins. Its short spines are harmless, but its pedicellariae, which look like small flowers, are tiny claws (Toxopneustes means “toxic foot”) containing a toxin that can cause severe pain similar to that of a jellyfish sting, faint giddiness, difficulty breathing, slurred speech, generalized weakness, and numbness of the lips, tongue, and eyelids.
Seafood poisonings are illnesses caused by ingestion of a natural toxin present in seafood. This toxicity can be inherent to the species — as is the case in fugu and other tetraodontiforms — or toxicity can result from external contamination, such as shellfish poisonings or ciguatera. Many gastrointestinal issues commonly attributed to seafood poisonings are often actually the result of gastrointestinal infections caused by ingestion of harmful bacteria, parasites or viruses, and for that reason they are not included in this text.
In this section we will discuss ichthyosarcotoxisms, forms of food poisoning resulting from ingestion of fish flesh containing natural toxins. Ichthyosarcotoxism originates from the Greek words ichthys (fish), sarx (flesh) and toxikon (intoxication or poisoning). The three main ichthyosarcotoxisms are ciguatera, scombroid fish poisoning and tetrodotoxism. We will also cover shellfish-related intoxications, but these cases cannot be called an ichthyosarcotoxism because shellfish are bivalve mollusks and not fish.
Ciguatera is caused by ingesting fish contaminated with certain toxins collectively known as ciguatoxins, which are produced by photosynthetic unicellular dinoflagellates (Gambierdiscus toxicus) that are part of phytoplankton. Dinoflagellates are epiphytes that live on macroalgae and dead coral surfaces. Small reef fish feed on these corals and macroalgae, accidentally ingesting these dinoflagellates. As larger predators eat the smaller fish, the toxin transmits up the food chain and accumulates in the tissues of top predators through a process known as bioaccumulation. Human poisoning can potentially occur when any of the fish involved in this chain are consumed, but poisoning is much more likely when eating the larger predators.

Species known to be a source of intoxication include barracudas, snappers, moray eels, parrotfish, groupers, triggerfish and amberjacks, but other species have been known to cause occasional outbreaks. Ciguatoxins, which rarely contaminate pelagic fish such as tuna, marlins, dolphinfish or other ray-finned fish, can be found around the world in the tropical reef belt between 35 degrees north latitude and 35 degrees south latitude.
Ciguatera is probably the most common type of marine food poisoning. Endemic in Australia, the Caribbean and the South Pacific islands, ciguatera cases should be naturally limited to those areas, but due to commercial imports cases have been reported in areas such as St. Louis, Missouri, and New York City.
Approximately 50,000 reported cases of ciguatera poisoning occur annually worldwide. Epidemiological data regarding ciguatera poisoning is challenging to collect; it is often misdiagnosed or undiagnosed because of the wide array of symptoms. People in endemic areas often disregard medical evaluation, while imported cases probably go undiagnosed or unreported because physicians outside of endemic regions may be unfamiliar with symptoms of a tropical toxin. Recent studies have suggested that the incidence of this illness is increasing, though this might be due to more reporting rather than an increased occurrence of the illness.
Toxicity depends on exposure and dose (how much is ingested), and symptom onset usually occurs two to six hours after ingestion. Symptoms can last for weeks to years and in some cases may lead to long-term disability.
Signs and symptoms can be highly variable but typically include neurological or gastrointestinal manifestations; about 80 percent of patients show varying degrees of impairment in both systems. The most common manifestations include the following:
There is no definitive treatment for ciguatera poisoning. Both first aid and hospital care are aimed at symptom control. If vomiting is profuse, it is important to prevent possible dehydration. If you suspect ciguatera, seek a medical evaluation. There are many folk remedies, but their efficacy has not been studied. The best course of action is prevention through education and avoidance of seafood in endemic or suspected areas.
The term ciguatera is actually inaccurate. Don Antonio Parra coined ciguatera in Cuba in 1787 to describe indigestion following ingestion of a type of marine snail called cigua (Turbo pica). It is unclear how the term cigua was transferred to an intoxication caused by the ingestion of coral reef fish.

Many different species of fish can be involved in scombroid poisoning, including mackerel, tuna, bonito, albacore, sardines, anchovies, mahi-mahi, amberjacks, marlin and herrings.
If these fish are poorly refrigerated after being caught, they will begin to decompose, and bacteria from their gastrointestinal tract will invade their flesh. Many fish contain a significant amount of an amino acid called histidine in their flesh. When decomposition begins, the bacteria from the gastrointestinal tract break down histidine into histamine (a small nitrogen compound involved in regulation of immune reactions and inflammatory responses). While ingestion of histidine is harmless, ingestion of large quantities of histamine can mimic an allergic reaction.
In the United States and Europe, scombroid fish poisoning — also called histamine fish poisoning — accounts for up to 40 percent of seafood-related foodborne illness outbreaks. Between 1998 and 2002, there were 167 reported outbreaks in the United States affecting 703 persons with no fatalities. Scombroid fish poisoning, which can happen anywhere susceptible fish are harvested, is more common when consuming fish caught recreationally or from small-scale operations; it rarely occurs in highly regulated fish harvests.
Ingestion of large quantities of histamine can mimic an allergic reaction. Symptom onset may range from minutes to up to two hours after consumption and typically resolves within 24 hours.

SYMPTOMS MAY INCLUDE THE FOLLOWING:
SIGNS MAY CONSIST OF THE FOLLOWING:
Due to its resemblance to an allergic reaction — and a poor awareness of intoxication — scombroid fish poisoning is commonly misdiagnosed as a seafood allergy. Anyone showing signs and symptoms compatible with allergic reactions should seek an immediate medical evaluation because allergic and allergic-like reactions can be life-threatening.
As opposed to genuine allergic reactions, where the source of histamine is internal, treatment for scombroid fish poisoning does not require the use of corticosteroids or adrenaline (epinephrine). Instead, scombroid fish poisoning responds very well to oral antihistamines, typically showing positive results within 10 to 15 minutes.
Never assume oral antihistamines are enough to control a presumed scombroid fish poisoning on your own. Always seek a professional medical evaluation, and let a medical doctor decide the treatment and best course of action.

Red tide is a colloquial term for a harmful algal bloom. Large concentrations of aquatic microorganisms occasionally bloom naturally in coastal areas. The rapid accumulation of algal blossoms can be significant enough to cause a green, red or brown discoloration of estuarine and freshwater environments. Scientists discourage use of the term red tide, because these phenomena are unrelated to tidal water movements and may not necessarily be red in color or present any discoloration at all. When these algal blooms are associated with potentially harmful toxins, the favored terminology is harmful algal bloom (HAB).
Among the involved microorganisms, certain species of phytoplankton may be present, which can produce harmful natural toxins that can become concentrated in tissues of filter feeders such as shellfish and other mollusks and crustaceans. The whole food chain may be affected, and millions of fish may die as a result.
These toxins can affect commercial fisheries and represent a public health threat. People who consume contaminated shellfish may suffer a variety of shellfish poisonings, some of which are potentially lethal. Hazards related to HAB may not be limited to shellfish consumption, so avoid harvesting any type of seafood in areas where HAB is known to have endemic outbreaks.

Shellfish are bivalve (two-part shells) mollusks that capture nutrients by filtering water. During this process, these filter feeders can accumulate toxins and other contaminants. When humans consume these bivalves, they may be poisoned. These toxins are water-soluble and heat- and acid-stable — they are unaltered by ordinary cooking methods. Shellfish poisonings are a group of four different syndromes caused by eating bivalve mollusks contaminated with toxins produced by microscopic algae.
Four different types of shellfish poisonings are primarily associated with mollusks such as mussels, clams, oysters and scallops.
These mollusks can accumulate a toxin called saxitoxin, which is produced by phytoplankton (dinoflagellates, diatoms and cyanobacteria). Some shellfish remain toxic for several weeks, while others can store the toxin for up to two years.

PSP blooms are associated with harmful algal blooms, which can occur in almost all oceans. PSP can be fatal, particularly in children. Symptoms, which can appear a few minutes after ingestion, include nausea, vomiting, diarrhea, abdominal cramps, numbness or burning around the mouth, gums, tongue and progressing to the neck, arms, legs and toes. Other symptoms may include dry mouth, shortness of breath, slurred speech and loss of consciousness. Signs of toxicity and mortality are also seen in wild animals.
This rare syndrome is caused by consuming shellfish contaminated with a toxin called domoic acid, produced by certain marine diatoms.
Symptoms, which can appear 24 hours after ingestion of contaminated mollusks, may include nausea, vomiting, diarrhea, abdominal cramps and hemorrhagic gastritis. Neurological signs include dizziness, disorientation, visual disturbances, short-term memory loss, motor weakness, seizures, increased respiratory secretions and life-threatening dysrhythmias (irregular heartbeat); these signs can be severe and may take up to three days to develop. Death is rare. Conditions resulting from permanent damage to the central nervous system may include short-term memory loss and peripheral neuropathy (weakness, numbness or pain as a result of nerve damage).
Certain dinoflagellates produce a toxin known as okadaic acid, which can damage the intestinal mucous membrane, making it very permeable to water, causing significant diarrhea as well as nausea, vomiting and abdominal cramps. Symptoms can strike within a few minutes to an hour after ingesting contaminated shellfish and can last for about one day. No life-threatening symptoms have been recorded, but serious dehydration may occur.
A dinoflagellate known as Karenia brevis naturally produces a toxin called brevetoxin, which can cause a variety of neurological symptoms similar to ciguatera. NSP is generally not life-threatening, but hospitalization is recommended until all other possible causes have been ruled out. In the United States and the Gulf of Mexico, a blossom of Karenia brevis usually causes HAB.
Treatment is symptomatic. Some cases may require hospitalization. If you think you or someone you know might have been poisoned after eating any type of shellfish, immediately seek an evaluation at the nearest emergency medical facility. Nonmedical personnel should focus on prevention.
DAN Boater encourages all travelers to get first-aid training so they are prepared to respond to diving or aquatic injuries, including marine life injuries. The following section details some of the first-aid techniques and treatments mentioned throughout the book, including thermolysis, antivenoms and the pressure immobilization technique. It is important to emphasize, however, that reading and understanding these materials is not a substitute for first-aid training.
If you have not been formally trained, DAN Boater highly recommends that you find a qualified instructor. To find a First Aid for Hazardous Marine Life Injuries instructor, visit DAN.ORG/Training/Directory.
The standard recommendations for toxin denaturation as a first-aid measure call for immersing the affected area in hot, fresh water with an upper limit of 113°F (45°C) for 30 to 90 minutes. This may work reasonably well when the toxin inoculation is skin deep, such as with a jellyfish sting, but it will be less effective when toxins have been inoculated by means of deeper puncture wounds, as with lionfish spines. Applying higher temperatures at skin level in an attempt to reach the desired temperature at a deeper level poses an unacceptable risk of burning the skin. In addition, vasodilatation caused by exposure to elevated temperatures may expedite the onset of distribution and of systemic effects.
Each case is unique and requires some estimation of the depth to which the venom was injected; for superficial inoculations, applying heat might be useful to manage pain and denature toxins, whereas for deeper inoculations, heat is only for pain management.
If you attempt to use thermolysis as a first-aid measure, minimize the risk of local tissue damage to the injured person by testing the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as intense pain may impair his or her ability to evaluate tolerable heat levels. Use the hottest temperatures you can tolerate without scalding. Note that different body areas have different heat tolerances, so test the water on yourself on the same area where the victim was injured.

Used in the treatment of venomous bites or stings, antivenom (also known as antivenin or antivenene) is a blood-derived biological product developed by injecting an animal — typically a horse, goat or sheep — with sublethal doses of venom. The animal will gradually develop antibodies against the venom, which can then be extracted from its blood as a serum to be administered to humans. Like most blood-derived products, antivenoms require an unbroken cold chain (proper refrigeration from production through storage until administration).
Though generally not a concern for first responders, administering antivenoms is not free of risk. Intravenous administration of animal serums can cause anaphylactic shock in susceptible individuals.
Conceptually, antivenom autoinjectors would work similarly to the way epinephrine autoinjectors (like EpiPen®) work for intramuscular administration. Though it is certainly a compelling idea, antivenoms are much more complex blood-derived products than epinephrine.
As such, they have a much shorter shelf life and require an unbroken cold chain. In addition, antivenoms are administered intravenously, a skill beyond that of first-aid responders. These limiting factors make this idea relatively impractical for field operation.

Use an elastic bandage and splinting to administer proper pressure and immobilization. An inelastic cloth is not ideal because it is difficult to achieve optimal pressure.

Since its inception in 1980, DAN® has spent more than 300,000 medical resource hours on duty, fielding more than 100,000 emergency calls and coordinating more than 10,000 emergency evacuations worldwide, making it one of the world’s most trusted resources for traveler safety.
As a natural evolution of DAN’s successful 35+ years of service to the diving community, our new DAN Boater membership program is committed to helping recreational boaters in need of emergency assistance while traveling the globe, and to promoting smart travel health and safety practices through research and education.
By boat, plane, car, or rail. Around the world, or across the state. Anytime you travel more than 50 miles from home, rely on DAN Boater for the assistance you need when you need it:
Learn how our affordable annual travel safety membership helps thousands of travelers just like you every day.